
Until recently, surgical excision was the only option to remove thyroid nodules. In the past, thyroid supplement medications had been prescribed with the hope of shrinking thyroid nodules, but the practice has been abandoned because it was not very effective. Though surgery is considered safe, it is not without risk to the nerve which controls the vocal cord, or a cosmetically unacceptable incision at the base of the neck. When half of the thyroid gland is removed, approximately 20% of patients will need thyroid supplementation afterwards and unfortunately there is no way to gain back thyroid function after it has been lost.
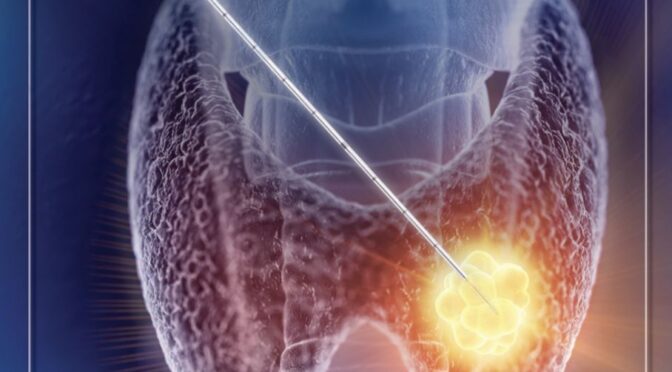
Radiofrequency ablation (RFA) is a new technique of shrinking thyroid nodules with less risk than surgery. The procedure uses a hand-held electrical device which is manipulated into the nodule under direct sonographic visualization. The procedure is performed in the office under oral sedative medication and local anesthetic.

Radiofrequency energy uses very rapidly oscillating electrical current to disrupt the cells and molecules within the nodule. This particular RFA device has a specialized temperature monitoring and cooling system to ensure no collateral injury to surrounding tissue or nerves occurs. RFA technology has been in use in medicine for decades, but this improvement in the instrumentation has allowed its application to the treatment of thyroid nodules.
This technique is supported by strong evidence for treating symptomatic or visible benign thyroid nodules. The data is also strong for treating toxic (overactive) thyroid nodules and even low risk papillary thyroid carcinomas measuring 1 to 1.5 cm or smaller in size.
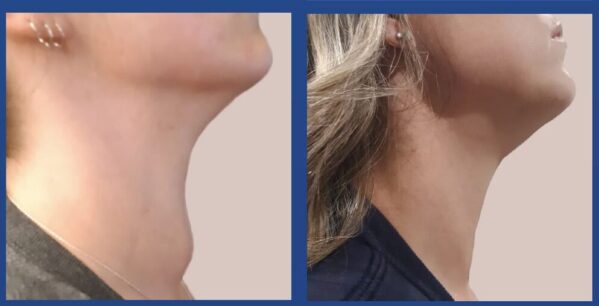
Over the counter pain medication is all that is needed afterwards for pain control, and there is virtually no downtime from normal activity. Perhaps most importantly, radiofrequency ablation can limit the need for thyroid surgery, which allows patients to keep their thyroid and reduce the risk of needing to take thyroid supplements.
Patients are carefully selected for this procedure. An ideal candidate for RFA has symptomatic or visibly conspicuous benign nodules. Two benign fine needle aspiration biopsies are recommended prior to the procedure. Fine needle aspiration biopsies, supplemented with a molecular marker analysis on indeterminate nodules allows proper candidate selection. A baseline ultrasound done in the office measures the size of the nodule, and imaging is repeated at scheduled intervals to assess the response. Very large nodules may require a second treatment after at least 6 months.
For patients travelling to Atlanta for RFA, a local overnight stay after the procedure is recommended.
Insurance Coverage
Currently, most insurance companies are not covering this procedure because it has no specific CPT (Current Procedural Terminology) code. Although there is robust data to support its efficacy and safety, they consider it experimental or investigational and do not guarantee payment. Unfortunately, we must collect payment in advance, but we will help you submit all the necessary paperwork to your insurance company to maximize your chances of being reimbursed.